
Why IGF-1 Bloodwork Doesn’t Always Tell The Whole Story

Everything below is for research and educational purposes only. Nothing here is medical advice.
The Measurement Gap
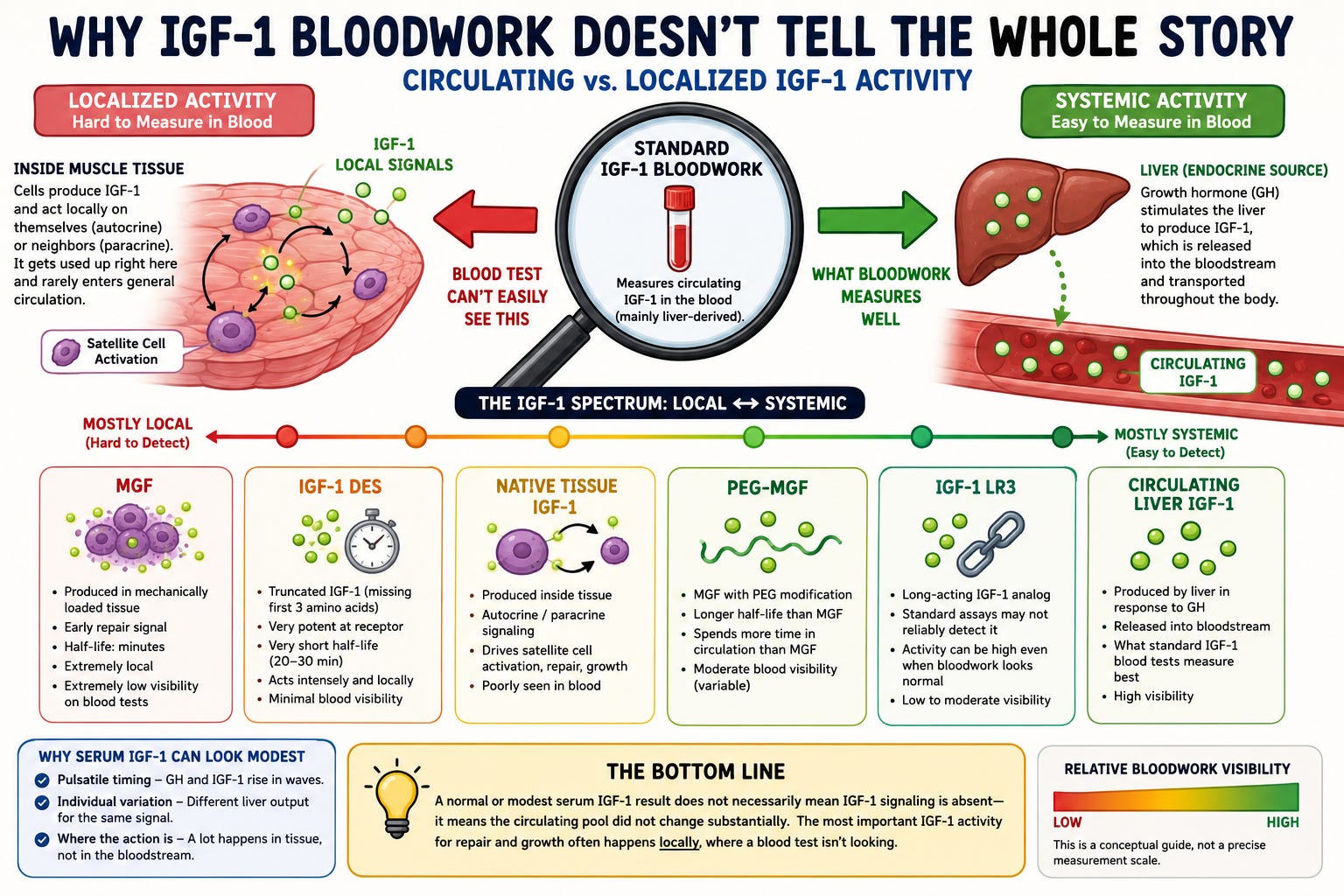
A standard IGF-1 blood test measures one thing well: the IGF-1 circulating in the bloodstream. That’s a real and useful signal, but it’s only one window into a system that operates in more than one place. A large share of IGF-1 activity happens in tissue, locally, where a blood draw was never designed to capture it. Understanding that gap is the difference between reading the number as the whole story and reading it as one data point among several.
What The Blood Test Actually Measures
When IGF-1 is tested, what’s being measured is circulating IGF-1. This is the IGF-1 the liver produces in response to growth hormone, released into the bloodstream, and carried around the body bound to its binding proteins. That’s the systemic, endocrine pool. It’s the version standard assays were built to detect.
But IGF-1 doesn’t only work as a hormone traveling through the blood from one organ to another. It also works locally, right where it’s made, and that local activity is largely invisible to a serum test.
The Part The Blood Draw Misses
IGF-1 has two modes of action beyond the systemic one, and both happen at the tissue level.
The first is autocrine signaling, where a cell produces IGF-1 and acts on itself. The second is paracrine signaling, where a cell produces IGF-1 and acts on its immediate neighbors. In both cases the IGF-1 is made, used, and consumed locally. It does its job right there in the tissue and never enters general circulation in a way that meaningfully changes the number on a panel.
This matters enormously for muscle. Under mechanical load, muscle tissue itself produces IGF-1. That locally produced IGF-1 drives satellite cell activation, repair, and growth directly in the worked tissue. It’s arguably the most relevant IGF-1 for the outcomes people care about, and it’s the pool a blood test is worst at seeing.
So local IGF-1 activity can be driving real change in the tissue while circulating IGF-1 looks flat. The signal that matters most for repair and growth is happening exactly where the blood test isn’t looking.
Why The Systemic Number Can Stay Modest
There are a few honest reasons the serum number can look unimpressive even when IGF-1 signaling is active:
Timing. GH and IGF-1 move in pulses, not a flat line. GH is released in bursts, and the IGF-1 response is delayed and smoothed out over time. A draw taken at the wrong point doesn’t reflect the real pattern.
Individual variation. Liver output of IGF-1 in response to a GH signal varies a lot from one individual to the next. The same input can produce different circulating numbers.
Where the action is. Some of the downstream IGF-1 effect plays out in tissue rather than as a large change in the circulating pool.
A flat or modest number tells you the circulating pool didn’t move much. It does not tell you that nothing happened at the tissue level.
The Full Picture
The serum IGF-1 number is one data point, and it’s worth tracking, particularly for safety, since chronically elevated systemic IGF-1 carries real proliferation considerations. But it should be read alongside everything else the system is showing, not treated as the single verdict. When tissue-level activity and a circulating number point in different directions, that’s not a contradiction to resolve in favor of the number. It’s a reminder that the number only ever described one of the two pools.
Why IGF-1 LR3 Is Interesting Here
This is exactly where IGF-1 LR3 becomes interesting from a measurement standpoint.
IGF-1 LR3 is a modified, long-acting analog. It’s structurally different enough from native IGF-1 that standard assays don’t reliably detect it. So the situation that’s already true for native local IGF-1, where activity outruns what the blood test captures, becomes even more pronounced. The bloodwork can come back looking unremarkable while IGF-1 signaling is present.
And there’s a second layer. Where the analog ends up matters. If it distributes systemically, it behaves more like a circulating factor and contributes to the body-wide pool, with all the body-wide considerations that come with elevated IGF-1. But if the activity is concentrated locally in tissue, that’s the same blind spot again. Native local IGF-1 doesn’t show up well on a serum test, and a localized analog effect is no easier to capture.
Put those together and you have a compound whose activity is genuinely hard to read off a blood panel. That’s part of what makes it scientifically interesting, and it’s also why the measurement limitation deserves real respect. A number you can’t see isn’t a number you can manage against.
The Other Variants Tell The Same Story
LR3 isn’t the only place this shows up. The wider IGF-1 family makes the circulating-versus-localized distinction even clearer, because several of these variants are defined precisely by acting locally rather than systemically.
IGF-1 DES is a truncated form of IGF-1, missing the first three amino acids. That small change makes it considerably more potent at the receptor and strips away most of its interaction with binding proteins. But the defining feature for this discussion is its very short half-life, on the order of 20 to 30 minutes. A short half-life is usually thought of as a limitation, yet it’s exactly what makes the molecule’s effect local in character: it acts intensely wherever its concentration is high and then clears before it can build into a meaningful, sustained systemic pool. The action is concentrated and brief, which is the opposite of the steady circulating presence a serum test is built to measure. A compound that does its work in a short local window and then disappears is, almost by definition, one that won’t paint a clean picture on a blood panel.
MGF, mechano growth factor, makes the point even more directly, because it’s something the body already produces on its own. MGF is a splice variant of the IGF-1 gene. Under mechanical load, muscle tissue reads that same gene differently and produces MGF instead of standard IGF-1. It’s the local first responder, produced right in the worked tissue, associated with the early phase of repair and with activating satellite cells before systemic IGF-1 takes over. This is native, endogenous, local IGF-1 signaling in its clearest form, and it’s the textbook example of activity that a systemic blood draw was never going to capture. Compounding that, unmodified MGF has a half-life of only minutes, so even the small amount that might reach circulation is gone almost immediately.
PEG-MGF is the modified version, MGF with a polyethylene glycol chain attached. The PEG protects the molecule from rapid degradation and slows its clearance, stretching the half-life from minutes to hours and allowing it to distribute more systemically than native MGF ever could. That makes PEG-MGF an interesting middle case for this exact theme: pushing the molecule toward systemic distribution makes it more present in circulation, while the native, unmodified form it’s based on is one of the most local, least measurable signals in the whole family. The same underlying molecule sits at very different points on the local-to-systemic spectrum depending on whether it’s been modified, and where it sits is precisely what determines how visible it would be to a measurement built around circulation.
The throughline across DES, MGF, and PEG-MGF is the same one that runs through native local IGF-1 and through LR3: the more a variant’s activity is concentrated locally and briefly, the less a circulating measurement captures it. Systemic presence and local action are different things, and the assay only sees one of them.
The Bottom Line
IGF-1 isn’t only a hormone in the blood. It’s also a local signal made and used inside tissue, and that local activity is a large part of repair and growth, especially in muscle. A standard blood test captures the circulating pool well and the local pool poorly.
So a flat or modest IGF-1 number doesn’t establish that nothing is happening. It establishes that the circulating pool didn’t move much. The tissue-level story is a separate one, and the blood draw was never the right tool to tell it. The variants make the same point from the other direction: DES and native MGF are defined by acting locally and briefly, LR3 evades the standard assay outright, and PEG-MGF only becomes more measurable to the extent it’s pushed toward circulation. Where a signal sits on the local-to-systemic spectrum is what decides whether a blood test can see it at all.
So does it even make sense to test IGF-1, or is there a better test?